Causes of Skin Changes in Leukocytoclastic Vasculitis

Illustration by Julie Bang for Verywell Health
Medically reviewed by Casey Gallagher, MD
Leukocytoclastic vasculitis, also known as hypersensitivity vasculitis, involves inflamed small blood vessels. It is not a disease. It occurs with many types of ailments.
About half of these cases occur without a known cause. The other 50% of cases are linked to a wide range of causes, such as drugs, food, infections, and chronic ailments. The problem can be confined to your skin, or it can worsen to involve your organs. The lesions can be acute or chronic.
Common symptoms include palpable purpura (purple-red raised lesions) often found on your legs. A skin biopsy is used to confirm the problem. More tests may be used to rule out systemic causes.
This article describes leukocytoclastic vasculitis causes, symptoms, testing, and treatment. It also includes tips for self-care.
Leukocytoclastic Vasculitis Related to Medication
About 10% of leukocytoclastic vasculitis cases develop as a result of reactions to medications. The amount of time between exposure to the medication and a reaction can range from hours to years.
Most cases of drug-induced leukocytoclastic vasculitis occur within seven to 21 days after starting a drug, increasing the dosage, or restarting a drug after having stopped it.
The following drugs are those most often responsible for causing leukocytoclastic vasculitis:
Antibiotics: Particularly sulfonamides, quinolones, beta-lactam antibiotics
Certain immunosuppressants: Neoral, Gengraf (cyclosporine), Imuran, Azasan (azathioprine)
Jylamvo, Trexall (methotrexate): A chemotherapy drug
Zyloprim, Lopurin (allopurinol): A uric acid reducer
Antithyroid drugs, particularly Propycil (propylthiouracil)
Certain antiepileptic drugs: Depakote, Depakene (valproic acid), Dilantin (phenytoin)
Antitumor necrosis factor-α agents: Immunosuppressant drugs
Apresoline (hydralazine): Hypertension (high blood pressure) drug
Nonsteroidal anti-inflammatory drugs (NSAIDs): Bayer, Ecotrin, Bufferin (aspirin), Motrin, Advil (ibuprofen), Aleve, Naprosyn (naproxen), Mobic (meloxicam), Celebrex (celecoxib), Indocin (indomethacin)
Learn More: Safer Alternatives to NSAIDs
Leukocytoclastic Vasculitis From Another Condition
While the cause of leukocytoclastic vasculitis is unknown in almost half of diagnosed cases, the condition is linked to several diseases that involve your immune system.
Some of the most common conditions linked to leukocytoclastic vasculitis include the following:
Infections, especially upper respiratory infections
Inflammatory bowel disease (IBD): Crohn's disease, ulcerative colitis, indeterminate colitis
Malignancy (cancer), though less often than other conditions
Generally, leukocytoclastic vasculitis is not life-threatening. Overall survival is good, averaging 99% at one year and 83% at three years, even in chronic cases. When a systemic disease is involved, your prognosis depends on the extent of organ involvement and the severity of the underlying condition.
Learn More: An Overview of Vasculitis
What Does Leukocytoclastic Vasculitis Look Like?
Leukocytoclastic vasculitis causes lesions that appear when damaged blood vessels leak, and small areas of hemorrhage appear as blood spots under your skin. The growths may occur alone or as grouped rashes.
Cutaneous (skin) leukocytoclastic vasculitis skin typically has the following appearance:
A new rash with tender purple or brownish-red purpura (bruise-like spots of blood under your skin) spread over large areas that usually develops over a few hours
Non-blanching characteristic (rashes that do not disappear with pressure)
Sores concentrated on your legs, trunk, or buttocks and less frequently on your forearm, and hand
Urticaria (hives) that can last longer than 24 hours
Blisters on your skin
Deep skin necrotic ulcers (open sores with dead tissue)
Petechiae (pinpoint purple or red spots)
Purpuric macules (purplish, irregularly shaped lesions)
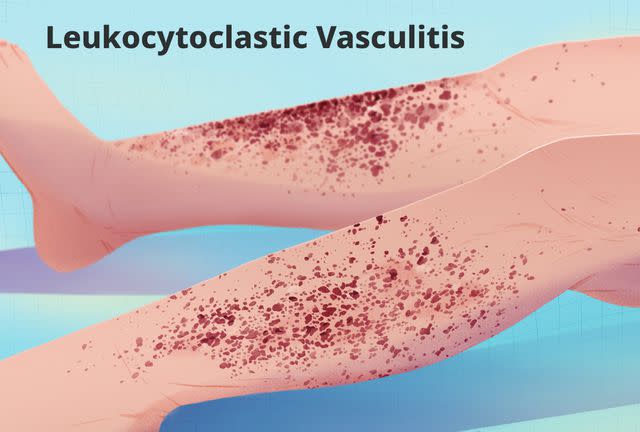
Illustration by Julie Bang for Verywell Health
How Does Leukocytoclastic Vasculitis Feel?
Leukocytoclastic vasculitis can be completely asymptomatic or cause a range of problems. Common symptoms can include the following in the involved skin:
Burning
Itching
Pain
When leukocytoclastic vasculitis is associated with systemic involvement, it can affect many different organs including your kidneys, central nervous system, heart, gastrointestinal tract, and lungs. The condition causes the following symptoms based on the organ involved:
Testing to Confirm Leukocytoclastic Vasculitis
Your healthcare provider will base the diagnosis of your symptoms on a series of tests to confirm a diagnosis of leukocytoclastic vasculitis. A skin biopsy is the gold standard for confirming a diagnosis.
The type of skin biopsy used is typically a punch biopsy. A punch biopsy uses a cookie-cutter-like skin punch to remove a sample of skin about the size of a pencil eraser. The biopsy removes deeper layers of skin, which are examined under a microscope to diagnose your rash.
Based on a comprehensive history and detailed physical examination, your healthcare provider will use one or more of the following tests to identify systemic conditions (those affecting one or more of the body systems) that may be the source of your symptoms:
Complete blood count (CBC) with differential
Erythrocyte sedimentation rate (inflammation test)
Antinuclear antibody (ANA)
Rheumatoid factor
Chemistry panel with liver enzymes and creatinine (a waste product in your blood and urine)
Antineutrophil cytoplasmic antibodies (ANCA)
Complement levels (test of a healthy immune system)
Cryoglobulins (abnormal proteins in your blood)
Differential Diagnosis of Leukocytoclastic Vasculitis
Leukocytoclastic vasculitis has a broad differential diagnosis, a diagnosis that considers and eliminates other possible causes of the symptoms and lab findings. It can be challenging to distinguish it from other causes of purpura. The extensive differential diagnosis of this condition includes the following:
Scurvy (vitamin C deficiency)
Ehlers–Danlos syndrome (connective tissue disorders caused by faulty collagen)
Non-LCV vasculitis (e.g., lymphocytic vasculitis)
Amyloidosis (the buildup of abnormal proteins)
Disseminated intravascular coagulation (a serious disorder of clotting and bleeding)
Thrombotic thrombocytopenic purpura (a rare blood clotting disorder)
Emboli (a mass, often a blood clot)
Pigmented purpuric dermatosis
Von Willebrand disease and other bleeding disorders
Thrombocytopenia (low platelet count, a blood cell involved in clotting)
Trauma
Does Treatment Cure Leukocytoclastic Vasculitis?
Treatment for leukocytoclastic vasculitis varies based on your history, the extent of the condition, and the underlying trigger. When a case of leukocytoclastic vasculitis is confined to your skin, the goal of therapies is to reduce inflammation.
Leukocytoclastic vasculitis generally has a good prognosis. Acute cases occur one time. They typically go away on their own over three to four weeks with or without treatment and do not recur.
Self-limited cases include drug-induced leukocytoclastic vasculitis. These cases typically improve with the discontinuation of the medication that triggered the reaction.
About 10% of cases involve chronic or recurrent disease. Chronic cases can occur when there is an underlying disease. Treatment for these cases involves getting an accurate diagnosis, starting the appropriate treatment, and maintaining disease remission to manage symptoms.
Medications to Control Leukocytoclastic Vasculitis
Medications to control leukocytoclastic vasculitis include supportive treatment with antihistamines and NSAIDs to relieve symptoms, but they do not alter the course of the disease.
When this condition causes severe and chronic symptoms or involves internal organs, treatment with systemic steroids alone or in combination with immunosuppressive drugs may be needed.
The following medications have proven effective in treating leukocytoclastic vasculitis:
Corticosteroids (prednisone or methylprednisolone)
Immunomodulators used when leukocytoclastic vasculitis involves systemic disease: Imuran, Azasan (azathioprine) with folate supplementation, CellCept (mycophenolate mofetil)
Self-Care With Leukocytoclastic Vasculitis
For cases of leukocytoclastic vasculitis confined to the skin, the following strategies are advised:
Rest (avoid prolonged standing or walking).
Elevate your legs when resting.
Wear compression stockings.
Apply ice packs to the affected area.
Wear loose clothing around affected areas.
For cases of leukocytoclastic vasculitis that involve chronic conditions, following recommendations for disease management and treatment as advised by your healthcare provider are important to control symptoms.
Summary
Leukocytoclastic vasculitis is a problem in which the small blood vessels in your skin are inflamed. Causes can involve drugs, food, or chronic conditions, though there is no known cause in about half of the cases.
Diagnosis of this problem can be a challenge. It has a broad differential diagnosis. While a biopsy is used to confirm it, finding its cause can involve many tests.
Symptoms appear as purple patches of raised lesions, often on your lower legs. More severe problems can occur if your organs are involved.
Treatment often involves easing pain and itching until the patches resolve. The prognosis for this problem is good. However, your outlook can change if it is caused by a chronic health problem that is not managed.

