This robot can perform soft tissue surgery better than a human

In a milestone that could pave the way for robotic surgery on humans, a robot successfully performed operations on four pigs. The findings are detailed in a study published Wednesday.
This advance in robotics comes courtesy of an enterprising team of surgeons and researchers at Children’s National Health System in Washington, D.C. and Johns Hopkins University in Baltimore, Maryland, who successfully built a new robo-surgical system and programmed it to suture together intestines.
The team’s work and eye-opening results are detailed in a new study, titled "Supervised Autonomous Robotic Soft Tissue Surgery," published Wednesday in the journal Science Translational Medicine.
Aside from the fact that a robot arm is autonomously performing surgery, the biggest breakthrough here may be that the robot, which they call “Soft Tissue Autonomous Robot” or “STAR,” was dealing with soft tissue.

Image: Sheikh Zayed Institute (SZI) at Children’s National Medical Center
“No one has ever done a soft tissue surgery in a robotic way — managing tissue that is deformable and mobile,” said study author and surgeon Dr. Pete C.W. Kim, who is a professor of surgery for the Sheikh Zayed Institute (SZI) at Children’s National Medical Center in Washington.
Traditional robot surgery tools like Intuitive Surgical’s da Vinci surgical system and Applied Dexterity’s RAVEN rely on human tele-operators controlling a cable-based system. Da Vinci doesn’t make decisions on its own, though it does stabilize the tools and even prevent tele-operators from cutting in the wrong place.
Even so, until now, no one has tried to let a robot perform surgery in these mine-field-like tissue areas without human intervention. And for good reason, Kim said that in a soft-tissue environment like the human abdomen, “everything is different shades of pink and shiny.”
In order for a true robot to autonomously deal with that kind of setting, the researchers had to build their own robot surgeon.
Robo-Surgeon
The STAR consists of a powerful, yet precise Kuka robot arm with seven degrees of freedom and a next-generation vision system comprised of both near-Infrared and a light field (or plenoptic) 3D cameras.
On the back end is programming that, to a certain extent, is like a surgical greatest hits of possible methods for rejoining dissected intestines, veins and arteries (eventually the system will have a vast knowledge base of surgical procedures, the researchers say). The process of reconnection is most commonly known as an anastomosis procedure. According to the study, roughly 1 million such operations are performed each year in the United States.
“We programmed the best surgeon’s techniques — based on consensus — into the machine… and the machine independently chooses the best ways to accomplish task,” said Kim.
The arm is built with a force system, to measure the suture tension, and STAR handles the miasma of pink with its super-vision.
To help the robot see, the human surgeon marks up key portions of the surgical area with bio-compatible markers so the near infrared camera can see them. That’s combined with the powerful light field camera for a view of the surgery a human could not duplicate.
“The promise of going hands-free has eluded soft-tissue, in particular because tissue is deformable,” said Science Translational Medicine senior editor Megan Frisk, during a press conference. “This represents a new era of robotic surgery.”
Under a watchful eye
Even though robotic, minimally invasive or laparoscopic surgery is fairly common today, it has not, according to Kim, radically improved surgical outcomes. “Even with minimally invasive techniques, complication rates have not really decreased,” said Dr. Kim.
The motivation for building STAR is to actually improve outcomes, he said, and part of that comes from a robot using the best possible surgical methods, even when the surgeon who perfected them isn’t there.
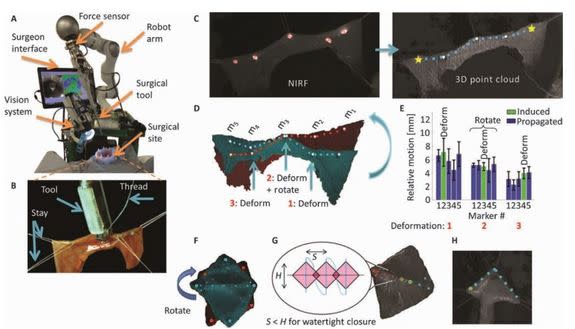
Image: SHEIKH ZAYED INSTITUTE (SZI) AT CHILDREN’S NATIONAL MEDICAL CENTER
Researchers actually performed two kinds of robot surgeries. One set took porcine intestinal tissue and secured it in a special ring, conducting the robotic surgery outside a living body. The others were performed on the live pigs.
Even though the robot performed the surgery, making each perfect suture in a fashion that actually outperformed those made by other systems and surgeons, researchers kept a human surgeon there to both serve as the other arm that kept stray sutures out of the way (a human surgeon does get to use two hands) and as a safeguard.
“It was a supervised autonomy,” said Ryan Decker, a co-author of the study.
“A surgeon oversees and has opportunity at any time... to stop the robot and take it out of scene — a finger-press away from taking it out of the surgery.”
The reality is, though, STAR robot’s sutures were so precise that, in post-operative tests, they held up better than those made by human hands.
Researchers performed a series of burst pressure or leak tests in which they took each sutured intestine — basically a tube — and pumped it full of air until it leaked. The robot sutures held up to higher pressures than those made by human surgeons.
How smart is it
The robot’s technique, though, is driven by skills that humans develop, and even though STAR chooses the best method for accomplishing a task, switching up methods as it goes along, it cannot learn new methods without additional programming.
“It has intelligence, but not a deep-learning neural network intelligence,” Kim said. “The idea is not to create a sentient being that completes surgeries.”
The team doesn’t want to replace surgeons.
“No matter where you are, you have access to best techniques and surgeons,” said Kim. “From surgeon’s perspective, why wouldn’t you want to have a tool that makes you better than what you are?”
And yet, the goal remains: unassisted robot surgeries.
“We can, in a relatively short period of time, be able to do an appendectomy, skin-to-skin, using current algorithm[s] and next generation of tools,” said Kim.
A robot surgeon looming over a patient without a human nearby to assist or hit the stop button may terrify some, but there are some obvious, far-reaching benefits.
To illustrate this point, Kim talked about SpaceX founder Elon Musk’s ongoing interest in traveling to Mars, a trip that could take 18 months each way.
Such a trip would take Musk beyond the bounds of tele-operation. Certainly today’s NASA astronauts traveling to the International Space Station or even a researcher about to be stationed in Antarctica for six months might see the benefit of a surgery robot stationed in a sterile medial pod, just waiting to perform the next emergency appendectomy.
Can we afford it?
While the research team wouldn’t offer any details on how much the STAR system costs, they said it should prove considerably less expensive than da Vinci, which is used to perform minimally invasive surgery (it controls tools through small incisions, basically ports, made to the body) and costs millions to buy and maintain. Also, unlike da Vinci, STAR’s hybrid makeup means that components like the Kuka arm could be easily switched out, especially as more intelligent and potentially cheaper robot arms become available.
The biggest savings, though, could come through value-based care, said Kim, who noted that robot surgery could “reduce complications and save money for the whole healthcare system.”
Even though STAR currently needs a human to, for instance, place the bio-markers, Decker said they’re already working on upgrading the vision system so the robot can do that on its own as well.
The STAR surgical experiments did take considerably longer than human ones, but Kim said they were not focused on speed for this proof of concept.
“We can run the robot really, really fast. In this study, we focused on the supervision and the outcome,” said Axel Krieger, who also worked on the study.
Even if hospitals and surgeons are not prepared to incorporate an entire robot system like STAR into their surgical wards, the researchers believe this robo-surgical solution will move quickly from research to commercialization.
“With the right partner, some or all of this technology can be incorporated into currently clinically available tools within next two-to-three years,” Kim said.
Dr. Benedict C. Nwomeh, a pediatric surgeon who has been using the da Vinci system for the last three years looked over the study for Mashable and offered these comments:
